Why the Elucid Model is Not Crop-Specific: Our 3-Pronged Approach for Health in Supply Chains

One of the most common misconceptions about Elucid is that we are a cocoa-focused company.
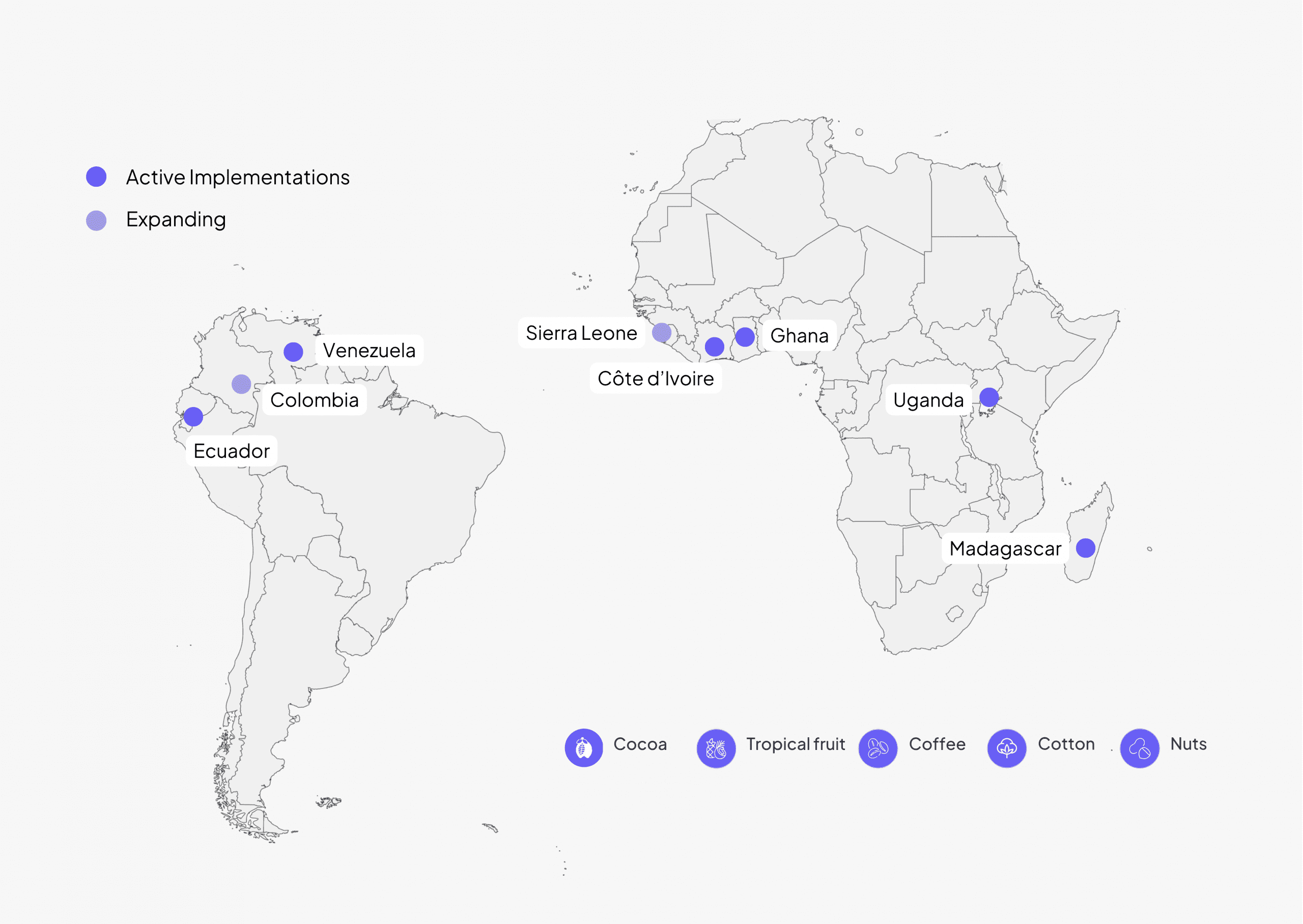
While cocoa has been a key entry point, our model is designed to operate across crops, geographies, and supply chains — from coffee and cotton to nuts and tropical fruits.
Why does it matter? Because supply chains rarely operate in isolation. Companies source across regions and commodities and need solutions that can operate consistently across them. Health needs may vary, but their impact on productivity, financial stability, and supply continuity is shared.
At Elucid, our work is designed to reflect that reality: embedding healthcare access, financial protection, and measurable impact across different supply chains, not just within a single pilot or geography.
In this article, we break down what makes that possible through three core elements: The Need, The Model, and The System.
The Need
Health needs exist across all supply chains, regardless of crop or geography. While the specific risks may differ, the underlying dynamic remains consistent: when health needs go unmet, they can disrupt farming households and the supply chains that depend on them.
Different crops come with different occupational health risks. In cashew farming, for example, exposure to cashew shell oil can lead to severe dermatological issues. In cotton farming, exposure to pesticides is associated with long-term conditions such as cancer and neurological disease. Farming practices, environments, and lifestyles vary — and so do the associated health risks.
But across these differences, the outcome is similar. Unmet health needs affect labour availability, reduce productivity, and place additional financial pressure on households.
As explored in our recent blog about health disruptions in supply chains, these effects extend beyond individual households — affecting productivity, financial stability, and broader production systems.
The need to address health in supply chains is therefore not crop-specific. It exists across contexts, sectors, and geographies. So, if the need is consistent, the question becomes: can the solution scale in the same way?

The Model
While contexts differ, the core of our model remains consistent and repeatable. Across every project, we follow the same structure to establish and scale access to healthcare.
Phase 1: Building the foundation for healthcare access. This includes:
- identifying and assessing local providers’ readiness;
- developing improvement plans to address infrastructure, service delivery, and staffing gaps
- mapping farming households within the supply chain
- conducting baseline assessments to understand healthcare needs
- designing and distributing training materials for both providers and farmers on the program and the digital platform
- training community agents and cooperative representatives to support onboarding and raise awareness
Phase 2: Scaling access to healthcare services. This includes:
- training healthcare providers to use our platform for real-time reimbursement processing
- enrolling farmers and their families onto the program and distributing membership cards
- running sensitization campaigns to support program navigation and awareness of healthcare benefits
- monitoring claims processing and healthcare utilization
- establishing healthcare facility improvement plans aligned with WHO quality standards
Across all contexts, these steps remain the same. What changes is the environment in which they are applied.
The strength of the model lies in its consistency: enabling comparable enrollment, financial protection, and measurable impact across different supply chains, while adapting to local needs and regulations.

The System
While the model remains consistent, healthcare systems vary significantly across countries and regions. This is why our approach is designed to complement, rather than replace, existing systems.
We work closely with national stakeholders, insurers, and healthcare providers to integrate with existing structures. These systems provide the foundation for implementation, and our role is to strengthen service delivery by addressing gaps where they exist. This includes aligning with national regulations, applying WHO-aligned quality standards, and coordinating with existing healthcare networks. By working within established systems, we avoid duplication and ensure that interventions are sustainable within the local context.
For example, in Ghana, we collaborate with the National Health Insurance Authority (NHIA) to enroll farmers into the existing National Health Insurance Scheme (NHIS), rather than creating a parallel system.

In addition, we share impact data with cooperatives and authorities to support decision-making and continuous improvement.
The system, in this sense, is the environment in which our model operates. While systems differ across contexts, the ability to integrate with them remains constant.
The Long and Short of It
The three elements – The Need, The Model, and The System – come together in different ways across projects, but they are always present.
The need for healthcare access exists across supply chains.
The model provides a consistent way to address that need.
The system determines how it is implemented in each context.
Together, these elements enable a replicable approach that can operate across crops, geographies, and supply chains — from local pilots to broader implementation.
As our work continues to expand into new sectors, this approach remains the same. Health is not tied to a single crop or context — and neither is the model designed to address it.
This is reflected in our ongoing expansion into new supply chains, including our first project in rubber in collaboration with the Global Platform for Sustainable Natural Rubber (GPSNR).
Related content
-
 We spoke with Jan Lühmann, a coffee consultant and our Topic Lead for Coffee. With decades of experience in the green coffee industry and sourcing regions around the world, Jan brings a practical perspective
We spoke with Jan Lühmann, a coffee consultant and our Topic Lead for Coffee. With decades of experience in the green coffee industry and sourcing regions around the world, Jan brings a practical perspective
-
 We often speak about resilient, strong supply chains at Elucid: specifically, how improving access to healthcare in smallholder farming communities contributes to that resilience. But what does that actually mean in
We often speak about resilient, strong supply chains at Elucid: specifically, how improving access to healthcare in smallholder farming communities contributes to that resilience. But what does that actually mean in
-
 Looking for a non-fiction read this summer? Interested in sustainable agriculture, supply chains, or global health? Over here at Elucid, we spent the week asking our team members and topic leads which books they
Looking for a non-fiction read this summer? Interested in sustainable agriculture, supply chains, or global health? Over here at Elucid, we spent the week asking our team members and topic leads which books they